

CMS Releases Post-ICD-10 Claims Denial Reimbursement Metrics
CMS has released new ICD-10 claims denial reimbursement metrics. CMS explains its evolving outlook and what comes next post-ICD-10.
Post-ICD-10 implementation claims denial is a top 2016 focus for healthcare organizations. According to last month’s ICD-10 survey from Porter Research and Navicure, healthcare organizations cite value-based care as a leading focus. Sixty percent of those surveyed saw no impact on monthly revenue post October 1, 2015. Revenue reportedly decreased by up to 20 percent for over one-third of participants.
Yesterday, the Centers for Medicare & Medicaid Services (CMS) released 2015 ICD-9 and ICD-10 Medicare fee-for-service claims rejection metrics. CMS outlined the key lessons learned over the past several months and provided an overview of claims submitted, claims rejected, and claims denied.
“This really is a new CMS,” stated Andy Slavitt, Acting Administrator of CMS, on the organization’s blog.
Although ICD-10 was once considered the Y2K of the healthcare industry, “the dire Y2K fears didn’t come to pass,” Slavitt said.
“On the big day, the ICD-10 Coordination Center was packed, and the CMS teams and our partners were geared up and ready to make sure that any burden on physicians could be minimized and concerns quickly addressed,” he explained.
Physicians, providers, hospitals, and healthcare organizations alike were all concerned about their revenue potentially dropping post ICD-10 implementation.
There was a high chance of aggressive private and public audits because of ICD-10’s increased coding specificity for healthcare providers and organizations, said George B. Breen and Bethany J. Hills, both Members of Epstein Becker & Green (EBG), the week before ICD-10 went live.
“Under ICD-10, the number of diagnostic codes available for coding healthcare services will go from 13,000 to 68,000,” they said.
“With more specificity, increased enforcement will likely follow. Healthcare entities should anticipate – and be prepared to respond to – aggressive payor audits, both private and public, in addition to enforcement efforts focused on whether clinical documentation supports the ICD-10 code selected, and the potential for claims of false or fraudulent billing when they do not,” Breen and Hills added.
This significant change was said to help the healthcare industry advance its nearly 30 year old, outdated administrative and operational processes.
“As a result of the replacement of the obsolete ICD-9-CM with the more modern ICD-10-CM and ICD-10-PCS code sets, patients can look forward to complete, accurate, up-to-date diagnostic and procedural data necessary to achieve significant advances in the quality of care and more efficient healthcare administrative processes,” stated the Coalition for ICD-10.
The coding transition came and went. Said Slavitt, CMS was well prepared to address claims denial issues and ensure uninterrupted reimbursement.
CMS valued the importance of continuing to learn more about the revenue cycle challenges small physician practices were struggling with, Slavitt said yesterday. CMS listened to concerns about claims payment concerns and cash flow, he added.
CMS utilized metrics that were, such as spreadsheets and scorecards.
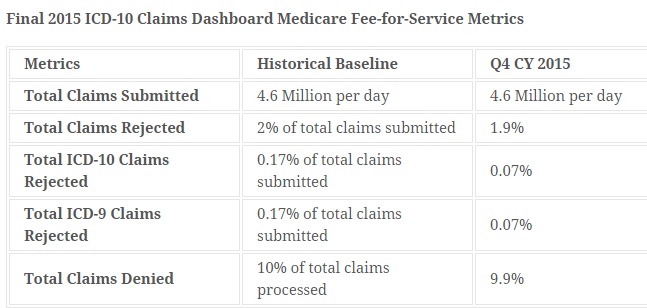
“Once we hit October 1, there were critical metrics to track. If doctors were sending us fewer claims, more claims than usual were denied, or a particular state was having trouble processing Medicaid claims, we needed to know as soon as possible.”
According to Slavitt, 4.6 million daily claims were submitted. Two percent of total claims submitted were rejected. The total number of ICD-9 and ICD-10 claims that were rejected each amounted to 0.17 percent, he said. The total number of claims denied was 10 percent of all processed.
But Slavitt said it is perhaps too soon to celebrate a low number of claims denials.
“With good implementations, we never declare victory and are still at the ready to continually improve,” he said.
“[Over] the next several years, we will be a part of implementing big and important changes that spend our health care dollars more wisely and keep people healthier – from how we pay for care to collecting and publishing data on how care is paid for to building consumer websites evaluating nursing homes to protecting beneficiary privacy and security,” Slavitt stated.
“Everyone saw the world hasn't ended because we're at ICD-10,” said Dave McCann, Managing Director at Berkeley Research Group’s Clinical Economics practice.”
“As long as they continue to monitor the documentation, the coding, and the billing, and then nip any problems in the bud, they're going to be just fine,” he asserted.
:ICD-10 has gone better than the worst-case scenarios people expected. They survived it. Now, they just have to keep moving, tracking, and improving.”
The next big focus needs to be on value-based reimbursement and value-based care. Healthcare organizations are honing in on where their reimbursement levels currently stand and how to maximize payment.
Post-ICD-10 two in three healthcare organizations plan to work on strengthening their general healthcare revenue cycle management processes, said Porter Research and Navicure.
Additional top 2016 focuses include migration towards one of many evolving value-based care models and automating and revising various patient collection strategies.
It is likely these will be big discussion points next week at HIMSS.
What’s next is exciting.
If the industry can handle ICD-10 claims denial management, it can essentially handle anything.
Source:http://revcycleintelligence.com/
.png)
